Recently the woman, who was a hospice nurse, had started caring for Kevin. Kevin had pancreatic cancer and lived alone in a house his sister rented for him. The sister never visited but held power of attorney. Given the man’s history of drug abuse, the nurse assumed the sister paid rent as penance for abandoning her brother to his addiction. But the nurse had made that up. She did that, tried to fit the puzzle pieces from the chart together into a coherent narrative.
The first time the nurse met Kevin, she feared him. She had read through his chart before that first visit, to prepare and saw that he had frequented a string of different doctors and pharmacies over the years in a shell game to get more opioids than any single doctor or any one pharmacy would give him. She read the previous nurse’s notes: “Patient raises his voice, states he is supposed to get more tablets, states, ‘I thought you guys were supposed to help me with my pain.’ Pt agitated, paces room.”
After that report, an electronic red flag appeared in his chart. A note by Kevin’s name said, “Do not visit this patient alone. Threatening behavior necessitates joint visits.”
Because of this, the nurse made her early visits with a social worker. From the start, Kevin did constantly pace around the room. He said he had “a lot” of pain, “ten or eleven out of ten,” he said. He cursed the agency, said no one cared. The nurse noticed that, in spite of his anger, he didn’t approach her or the social worker; he just paced and flapped his arms. He didn’t threaten. So the next visit she went alone.
This man never answered his door. Although only in his forties, he didn’t hear well and was asleep when she arrived. The nurse knocked hard at his kitchen entry and waited. She opened the door a crack and shouted his name. In the beginning that was enough, and he called back for her to come in.
As she stepped inside the home, the nurse tensed, wondering if coming alone was the right decision. She carefully followed the guidelines she had learned in nursing school: she didn’t let him get between her and the exit route. She hovered near the kitchen door. She watched his body language for signs of aggression or rising tension. Like the first time, he paced but he kept his distance. “You can come in,” he told her, gently, motioning to a chair. Fear recognizing fear. She stayed put.
“I want you to know,” she told him, “you are the boss of your body and your health. You make the decisions.” He stopped pacing, fidgeted with an empty paper bag on the dining room tabletop. She went on, “But I need you to communicate with me, OK? I’m not perfect, but if you tell me what you need, I will do my best to help you feel better.” He stopped fidgeting with the bag and met her eye for the first time.
“Okay,” he said. “Okay.”
At first she didn’t like Kevin much because he resisted her care, anyone’s care. No, he didn’t want oxygen to help him breathe. No, he didn’t want a walker so he wouldn’t fall. He wouldn’t let her listen to his chest, his heart, his flat belly. He didn’t want her to arrange a hired aide to clean up his kitchen where the counters were entirely covered with open, mostly empty, cans of soup, boxes of cookies, jars of applesauce, spaghetti sauce, peanut butter. Candy bars lay on the table, between sofa cushions, on the chairs. “I’m fine,” he said, “I just need to clean up a little. I’m lazy.”
Her first gift to him –the first tool to help him – was Oxycodone. He came to trust that she would bring the small white tablets in time, before the withdrawal symptoms set in – the sweating, the crawling sensation on his skin, before the pain caught up with him. A small trust. Routine for her: “Of course I will bring your medication exactly as I said I would.” But it mattered.
He still didn’t want her to touch him much or to stay long. He knew he had a weakened immune system so he was afraid of COVID. She worked as quickly as she could – opening the Fentanyl patch packages, peeling back the clear dressing, labeling the patches each with date and time. When she said she was ready, he turned his back to her and raised his T-shirt just far enough for her to see the old patches and peel them off. “Up a little higher,” she coaxed. He complied. She applied the new patches, covered them with the clear dressing. His flesh felt warm under her cool fingertips. “All set,” she said.
The next visit, the pain lines in his face had eased. He stood taller, his limp less pronounced. “It’s helping,” he said, “the medicine.” For a minute she could imagine him as a younger man – reckless and friendly.
“Good,” she said.
The junkies (“drug seekers,” as medical professionals called them) were never satisfied, in her experience. The nurse had cared for plenty of them. Their habits had left those people tolerant to huge doses of opioids with little effect. No matter what you did, they always described their pain as eight, nine, or ten out of ten. She assumed they had learned to say that to get more drugs. They said it even while outwardly showing no sign of discomfort – no furrowed brow, no rapid heartbeat or guarding. Sometimes they said it while so sedated they could hardly keep their eyes open. In those cases, she gave the medications as ordered by the doctors, larger and larger doses until the only thing that could dull the ephemeral pain was ketamine or midazolam, both so strong they were often used for surgery.
Many nurses and doctors resist giving people with a history of substance abuse large doses of opioids for their pain. They say the person is lying and just wants to get high. Which is sometimes true. But when you are dying, when a cancerous tumor grows larger, presses against muscles, organs and bones, the importance of your history fades. Any lies you have told, deceptions, family betrayals, all recede like the tide. What’s left is the pain. And the person.
Given this, it surprised her when she asked Kevin about his pain and he said, “I’m comfortable. It’s working.”
In her mind, she added, For now. Out loud she said, ”Good. Let me know at any time if the meds don’t manage your pain, OK?”
He said, “Yes,” and “Thank you.”
Kevin had an ex-girlfriend with whom he stayed close. She lived an hour or two drive away but she had driven over the day before. “I took her out for steak,” he said, “at the casino.” He lifted his chin when he said this, his dark eyes smiling.
Later that visit Kevin spent a long time looking out the window as the nurse packed her bag. The nurse followed his gaze. Behind the house, a raccoon shambled across unmowed grass.
“I want to trade places,” Kevin said without turning.
“With the raccoon?”
“He’s outside, wild.”
“Scrappy,” she agreed.
“He’s not scared of anything.” Kevin watched the animal disappear into a copse of cedar saplings.
This next time he was willing to talk about “poop.” They had to talk about it because opioids slow the bowels. Anyone who uses Fentanyl needs help. The nurse had been coaxing Kevin gently each week. She ordered an array of laxative choices for him – from the bitter sugary orange liquid to the chalky white powder to put in juice, from the acrid soda water that looked like Sprite to the slippery white pellets that go “in my asshole?” he said, incredulous. “No, I don’t think so.” He tossed the packet across the room.
“Just for an emergency,” she said. She couldn’t help laughing a little. She could do that with him now. “I know it sounds gross.”
“Oh, no. No, no, no.” He walked away as if escaping her reach.
“All my patients who’ve had it, say it isn’t bad, that it doesn’t hurt.”
He changed the channel on his TV, the screen as tall as he was. It sat directly across from the sofa where he spent most of his time under several blankets.
Just hang onto it, OK?” she said of the suppository. He didn’t answer.
But he did start the next visit with “the poop report,” proudly. “I had one today.”
“A BM?”
“Yep.”
“Excellent!”
“I know.”
He never let her listen to him with a stethoscope, and she stopped asking. One visit, though, he said, “Can you look at something?” He pulled his left pant leg two thirds of the way up the calf. The skin there was inflamed to the color of a ripe tomato. It had cracked open like dried mud to show fissures of moist pink flesh underneath. Clear fluid drained down into his sock.
Wounds fascinated the nurse. Each one was a puzzle to be solved. If you figured out the right steps, the right way to cleanse and dress it, the wound would stop hurting, stop stinking and weeping. Healing was one of the body’s many miracles. And, in her profession, she didn’t get to heal people often. Not physically.
She knelt in front of Kevin for a few minutes to examine the calf, then went back out to her car to gather supplies. This required removing her PPE. Once the acronym had been jargon used only by other medical professionals but in these days it of COVID, it came up regularly in newscasts and Twitter feeds. The nurse stripped off the paper gown and gloves, balled them neatly into an inside-out package, gelled her hands, removed her mask and goggles, gelled again. After collecting supplies from her trunk, she put fresh PPE back on. She feared she had taken too long and that Kevin would have changed his mind about letting her help. But he let her kneel again at his feet and wash the broken skin with sterile saline. She squeezed out medical honey onto a fabric mesh moistened with petroleum jelly. She flattened the sticky fabric against the open skin of his calf. He watched. Finally she wrapped the area with one long strip of white gauze and taped it into place. When she finished, he looked pleased. He said, “That’s better.”
Kevin got thinner. At her last visit before vacation, the nurse had to call louder and longer to get him to respond. She wondered if he had died. She pushed the door inward, walked into the kitchen, shouting his name. “Kevin. Kevin, it’s the nurse.”
When he finally woke, he staggered off the couch, disentangling himself from dark blankets. He stumbled as he got up, fumbling with his mask, a grubby black piece of polyester that gave him an animal-like muzzle. “You are coming today?” he said. He stood in the middle of the room, pants sagging around his narrow hips.
“That was our plan last week.”
“Oh. I didn’t know.”
The nurse wrote the date and time of his next visit, with a fill-in nurse, in large letters on a sheet of paper and set it on the little table where he ate.
When she finished that day, he said, “I appreciate your help. So much. Thank you.” His words followed her out the door. “Thank you.”
Back at work after her vacation, the nurse called Kevin before her next visit. As usual, he didn’t answer. She left a message.
The nurse approached Kevin’s door. This had all become familiar to her, including the way he draped an old blanket over and closed the door on it. She assumed he did this to fill the crack and keep the cold wind out. She knocked hard. The wood hurt her knuckles. “Kevin,” she called out, listened for movement inside. Heard nothing.
It felt intimate to open the door, as if she was a family member, and she liked that feeling. “Kevin?” she called again. “It’s me, the nurse.” She stepped inside. This is when he would usually start to respond. “Kevin, are you awake? It’s me.”
Nothing.
Something ticked against the sliding glass door that looked out into the forest. Through it she could see boughs writhing in the gusts. Small twigs flew through the air. Usually she would keep calling out but today felt different. She stood in the cluttered little kitchen, taking a moment before rounding the corner to see the sofa where he slept. As she waited, she saw the dark hulk of the raccoon outside. The animal glanced her way, meeting her eye, then ambled unhurriedly across the back yard, disappearing into the trees. It recognized her and was not afraid.
Monica Woelfel’s work has appeared in North American Review, The Seattle Review, Event, and The Sun. She holds an MFA in Fiction from University of British Columbia and lives in Bellingham, WA, where she works as a hospice nurse.
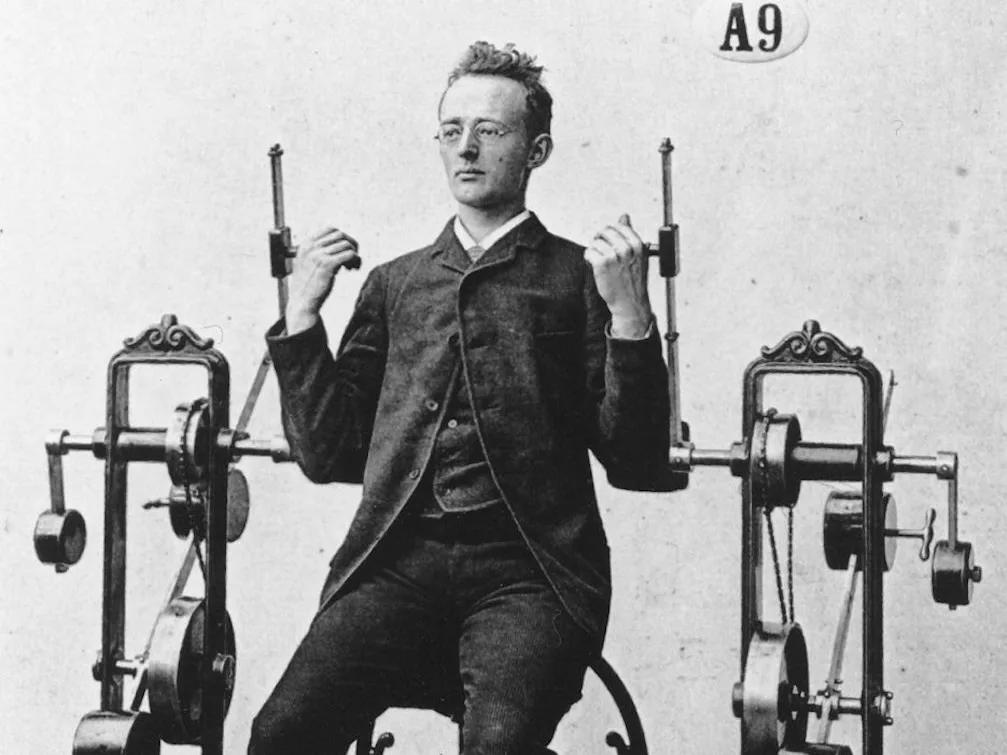
These images come from a catalogue distributed by “Görransson’s mekaniska verkstad”, a gymnastics equipment company, and are reproduced in a book published by Dr. Alfred Levertin on Dr. G. Zander’s Medico-Mechanische Gymnastik (1892). Aside from the shock of seeing the gymgoers’ choice of athletic wear (thick three-piece suits with pocket watches affixed on chains), there is something uncanny about the marked lack of exertion displayed on Zander’s patients’ faces. Zander’s technology was marketed as a passive activity — with some devices even driven by steam, gasoline, or electricity. All one had to do was connect their body to the machine and it would do the work for them. . . or so they were told.
From Public Domain Review: publicdomainreview.org/collection/zander-gym.
For more on Zander, see the article by Carolyn de la Pena at www.cabinetmagazine.org/issues/29/pena.php